
Can you ruck with arthritis?

It's a fair question - especially for older adults considering the sport for the first time, veterans managing wear-and-tear injuries, or anyone who's been told at some point to "take it easy on your joints."
The short answer is yes, in most cases. The longer answer is worth understanding.
Arthritis is not one thing
Before we talk about rucking, the word "arthritis" needs to be unpacked. It's an umbrella term covering over 100 conditions. For ruckers, two types are most relevant.
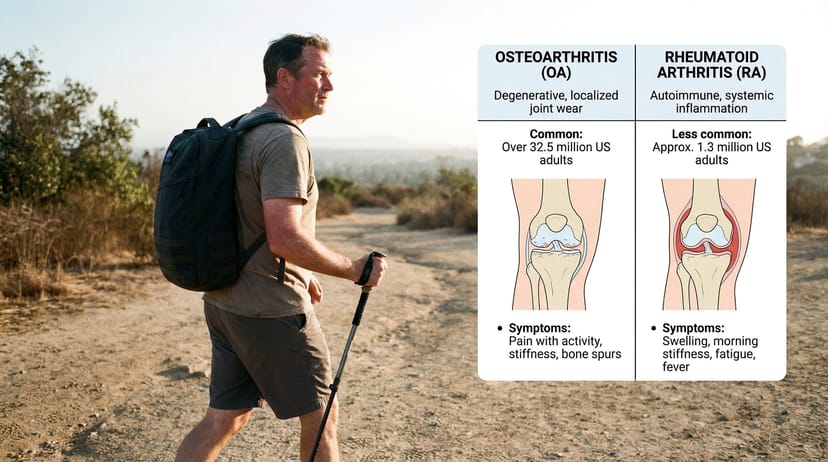
Osteoarthritis (OA) is the most common. It's the degenerative wear-and-tear version - cartilage between joints breaks down over time, leading to pain, stiffness, and reduced range of motion. It's most common in knees, hips, and spine. The majority of people asking about rucking and arthritis have OA.
Rheumatoid arthritis (RA) is an autoimmune condition where the immune system attacks joint tissue. It's systemic, affects multiple joints simultaneously, and comes with flares - periods of heightened inflammation that require a completely different approach than OA.
The research picture and practical approach differ significantly between the two, so knowing which you have matters before you do anything else.
What the research says about OA

Here's the counterintuitive thing about osteoarthritis: rest is not the answer.
Cartilage is avascular tissue - it has no direct blood supply. It receives nutrients primarily through diffusion from synovial fluid. Movement supports this process: mechanical loading stimulates chondrocytes (the cells that maintain cartilage) and multiple studies demonstrate that acute exercise upregulates amino acid metabolism in synovial fluid, helping replenish the building blocks cartilage needs. The relationship is not as simple as "movement pumps nutrients in" - but the net effect of appropriate loading on cartilage health is well-supported.
This is why long periods of inactivity tend to worsen OA symptoms over time. The joints stiffen, the surrounding muscles weaken, and the load-bearing demands on the cartilage itself increase because there's less muscular support around the joint.
A systematic review of exercise therapy for knee OA found pooled effect sizes of 0.52 for aerobic walking and 0.39 for quadriceps strengthening on pain reduction. Both approaches meaningfully reduce pain and disability - and both are recommended as first-line interventions by major rheumatology guidelines including the American College of Rheumatology. Walking of up to 10,000 steps per day does not appear to cause structural OA progression.
Loaded walking - which is exactly what rucking is - offers several specific benefits for OA:
Muscle strengthening. The quadriceps, glutes, and calves all take on extra demand when you add weight to your pack. Stronger muscles around arthritic joints consistently reduce pain and improve function - though the mechanism is more complex than simply "absorbing force." Multiple clinical trials show strength training improves pain and mobility in knee OA without necessarily changing the compressive forces measured during walking, suggesting benefits come through pain modulation, improved joint stability, and neurological adaptations rather than purely mechanical load reduction. The outcome is the same: less pain, better movement.
Weight management. Biomechanical research shows that each pound of bodyweight lost reduces the load on the knee by approximately four pounds per step during daily activities. Being just 10 pounds overweight adds 30 to 60 pounds of force to the knee with every stride. Rucking burns 300 to 600 calories per hour depending on weight and pace, making it an effective tool for weight management - which directly addresses one of the primary drivers of OA progression. Controlled trials show a 10% weight loss produces measurable reductions in knee joint compressive force.
Synovial fluid circulation. The rhythmic compression of walking keeps joint fluid circulating, delivering nutrients to cartilage and clearing out inflammatory byproducts.
Bone density. OA is sometimes accompanied by concern about bone health, particularly in older adults. Loaded walking is one of the most effective non-pharmaceutical interventions for maintaining and improving bone mineral density.
One important caveat: there is no peer-reviewed research specifically on rucking (loaded walking with a weighted pack) and arthritis. The evidence base here is exercise science for OA generally - walking, aerobic activity, and resistance training. Rucking sits at the intersection of all three, which is why the principles apply. But it's honest to say the research is on the category, not the specific activity. This is not a claim that rucking cures arthritis or reverses cartilage damage. The claim is more modest: controlled, progressive loaded walking can reduce pain, improve function, and slow progression for many people with OA. Whether it's appropriate for you specifically requires a conversation with your doctor.
What the research says about RA

Rheumatoid arthritis requires more caution and a more dynamic approach.
The general consensus in rheumatology supports regular low-to-moderate intensity exercise for RA patients - it reduces fatigue, improves mood, maintains joint function, and doesn't accelerate joint damage in controlled circumstances. But RA introduces a variable that OA does not: flares.
During an active flare, affected joints are acutely inflamed. Rucking through a flare - or any significant exercise through one - can worsen inflammation and delay recovery. This is not a "push through the pain" situation.
The approach for RA ruckers:
- Remission or low disease activity: Rucking can be appropriate with medical clearance. Start very light (5-10 lbs), short duration (15-20 minutes), and on flat terrain.
- Active flare: Rest the affected joints. Light walking without load is often acceptable if your doctor approves, but adding pack weight during a flare is not.
- Post-flare return: Treat it like returning from any injury. Drop back to your baseline load and duration, rebuild gradually.
RA medications also matter. Some immunosuppressants used in RA treatment affect how the body responds to exercise and infection risk. Your rheumatologist needs to be part of the conversation.
How to ruck with arthritis: practical framework
Assuming you have medical clearance, here's how to approach rucking with arthritis - specifically OA in weight-bearing joints.
Start lower than you think
For most ruckers, the starting recommendation is 10% of bodyweight or less. For ruckers with arthritis, start at half that. If you weigh 180 lbs, begin with 8-10 lbs, not 18.
Your joints need time to adapt to loaded walking - the muscles, tendons, and cartilage all respond to mechanical stress, but the adaptation timeline is longer with arthritis. A pack that feels light is doing the adaptive work without overwhelming the joint's capacity to recover.
Shorter, more frequent sessions beat long ones
A 20-minute ruck three times per week is a better starting point than a 60-minute ruck once a week. Shorter sessions keep total joint stress manageable, allow for recovery, and build the movement pattern consistently.
Progress to longer sessions only after the shorter ones feel fully comfortable - no increased pain, no significant stiffness the next morning.
Flat terrain first
Hills amplify compressive forces on arthritic knees and hips significantly. Start on flat pavement or soft track surfaces. Once you've built a base over 4-6 weeks, introduce gentle inclines.
Downhills are harder on arthritic joints than uphills. When you add terrain, pay more attention to how your joints feel on the descent. Trekking poles can take meaningful load off the knees on descents - the Black Diamond Trail Trekking Poles are a straightforward, affordable pair that many ruckers use specifically for downhill joint relief.
Footwear matters more than usual
For ruckers without arthritis, footwear is about comfort and stability. For ruckers with arthritis - particularly knee or hip OA - footwear can meaningfully affect the stress traveling up through those joints.
Look for shoes with good cushioning in the midsole, a stable heel counter, and a low-to-moderate drop (4-8mm for most people). Avoid maximalist cushioning that makes foot feedback hard to read - you want to feel what your foot is doing without absorbing excessive impact. The Salomon Quest 4 GORE-TEX is a representative example of a supportive midcut with a stable heel and moderate drop, which is the rough profile to look for.
Insoles designed for impact absorption can help. A sports medicine podiatrist can assess your gait and recommend orthotics if your walking pattern is placing asymmetric stress on one joint.
Read the signals correctly
Not all discomfort is a stop sign. Here's a rough guide:
Normal: Mild muscle soreness in the 24-48 hours after a ruck. Mild, diffuse joint aching that resolves within a couple of hours of finishing.
Slow down: Joint pain during the ruck that increases as you continue. Swelling during or immediately after. Pain that rates above a 3 out of 10.
Stop and reassess: Sharp, localized joint pain. Any pain above a 5 out of 10. Swelling that persists into the next day. Pain that changes your gait and causes you to compensate.
The rule that applies to all injury-adjacent rucking applies here: pain that changes how you walk is your body routing around a problem. That compensation creates new problems elsewhere. Stop, recover, and address the underlying issue before continuing.
Allow more recovery time
For ruckers without arthritis, 48 hours between sessions is a standard recovery window. With arthritis, build in 48-72 hours between sessions initially, and pay attention to how your joints feel 24 hours post-ruck rather than just during the activity. Some inflammatory response is delayed - what feels fine on the ruck may show up the following morning.
What rucking won't do
It's worth being clear about the limits.
Rucking will not regenerate cartilage. Cartilage degradation from OA is not reversible through exercise. The goal of exercise - including rucking - is to reduce symptoms, slow progression, improve surrounding muscle strength, manage weight, and maintain quality of life. That's a meaningful set of outcomes. It's just not a cure.
Rucking is also not a replacement for medical management of arthritis. If you're managing with medication, physical therapy, or other interventions, those continue. Rucking is additive, not substitutive.
The short version
Rucking is not off-limits with arthritis. For many people with osteoarthritis, controlled loaded walking is one of the best things they can do for their joints. For rheumatoid arthritis, it requires more care and tighter collaboration with your rheumatologist - but it's still on the table for most people in remission or with low disease activity.
The key variables are load, duration, terrain, and recovery. Start conservatively on all four. Progress slowly. Listen to your joints - not just during the ruck, but the morning after.
Get medical clearance before you start. That's not a liability disclaimer; it's genuinely good advice. A sports medicine physician or physiatrist who understands exercise-based management of arthritis is worth talking to. They can tell you specifically what's appropriate for your joint, your disease stage, and your current fitness level.
If you clear all of that - get outside and start walking. The research is on your side.
Frequently Asked Questions
Rucking is not inherently bad for arthritic knees. Uncontrolled, excessive loading is bad for arthritic knees. When properly dosed - light pack, flat terrain, gradual progression - loaded walking strengthens the muscles around the knee and can reduce OA symptoms over time. Medical clearance and conservative progression are essential.
Start at half the standard recommendation. If you weigh 180 lbs, the typical starting point is around 18 lbs - with arthritis, start at 8-10 lbs and build from there over several weeks. Prioritize duration and consistency over load increase.
For RA patients in remission or with low disease activity, regular low-to-moderate intensity exercise (including rucking) can reduce fatigue, improve mood, and maintain joint function without accelerating joint damage. During active flares, rucking should stop until the flare resolves. Always coordinate with your rheumatologist.
Mild aching that resolves within an hour of finishing is generally acceptable. Pain above a 3-4 out of 10 during a ruck, swelling, or pain that persists into the next day is a signal to stop and reassess. Sharp or localized joint pain is always a stop sign.
Look for stable, well-cushioned shoes with a moderate heel drop (4-8mm) and a firm heel counter. Avoid both minimal/barefoot shoes (too little protection) and extreme maximalist cushioning (too little proprioceptive feedback). A sports medicine podiatrist can assess your specific gait if you have persistent issues.



